
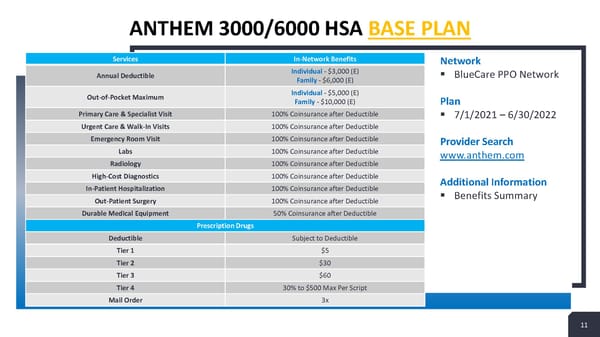
ANTHEM 3000/6000 HSA BASE PLAN Services In-Network Benefits Network Annual Deductible Individual - $3,000 (E) ▪ BlueCare PPO Network Family - $6,000 (E) Out-of-Pocket Maximum Individual - $5,000 (E) Family - $10,000 (E) Plan Primary Care & Specialist Visit 100% Coinsurance after Deductible ▪ 7/1/2021 –6/30/2022 Urgent Care & Walk-In Visits 100% Coinsurance after Deductible Emergency Room Visit 100% Coinsurance after Deductible Provider Search Labs 100% Coinsurance after Deductible www.anthem.com Radiology 100% Coinsurance after Deductible High-Cost Diagnostics 100% Coinsurance after Deductible Additional Information In-Patient Hospitalization 100% Coinsurance after Deductible ▪ Benefits Summary Out-Patient Surgery 100% Coinsurance after Deductible Durable Medical Equipment 50% Coinsurance after Deductible Prescription Drugs Deductible Subject to Deductible Tier 1 $5 Tier 2 $30 Tier 3 $60 Tier 4 30% to $500 Max Per Script Mail Order 3x 11 11
 Sample Open Enrollment Presentation Page 10 Page 12
Sample Open Enrollment Presentation Page 10 Page 12